Ureteral Pelvic Junction Obstruction (UPJO)
PREOPERATIVE EVALUATION
All patients are assessed preoperatively with a history, physical examination and diuretic renal scan, excretory urogram (IVP) and/or retrograde pyelogram. CT scan may also demonstrate the presence of a UPJO.
 Ureteral pelvic junction obstruction. Thirty-minute excretory urogram (EXU) demonstrating a normal left kidney and an obstruction of the proximal ureter (yellow arrowhead).
Ureteral pelvic junction obstruction. Thirty-minute excretory urogram (EXU) demonstrating a normal left kidney and an obstruction of the proximal ureter (yellow arrowhead).
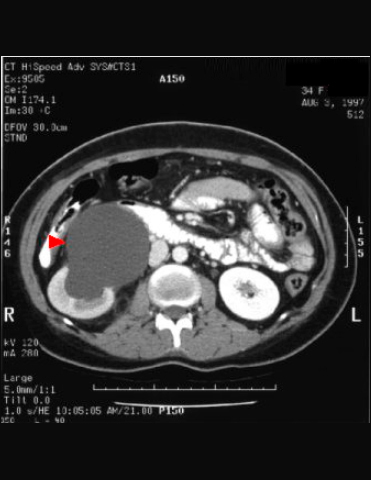 Ureteral pelvic junction obstruction. Early contrast enhanced CT scan demonstrating a normal left kidney and a dilated renal pelvis (red arrowhead).
Ureteral pelvic junction obstruction. Early contrast enhanced CT scan demonstrating a normal left kidney and a dilated renal pelvis (red arrowhead).
TREATMENT OPTIONS:
OPEN PYELOPLASTY
Open pyeloplasty has been the “gold standard” for surgical treatment of UPJO with a success rate of 90%.
Advantages: Neither the antegrade nor retrograde endourological approach achieves results to open pyeloplasty.
Disadvantages: Several draw backs, which include significant postoperative pain, prolonged convalescence and a prominent skin incision.
ENDOPYELOTOMY
An endoscopic approach to treating UPJO via an antegrade or retrograde approach.
hegrade endopyelotomy
A minimally invasive approach via a percutaneous nephrostomy tube that uses a hook blade to incise the UPJO. This approach has a success rate of 72-86%. The average operating time varies from 89.4 to 200 minutes.
Advantages
Disadvantages
Patients will have a nephrostomy tube postoperatively.
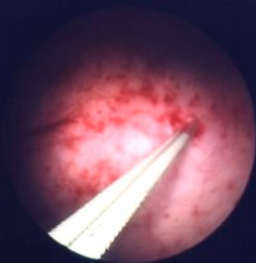
Retrograde endopyelotomy
Using a minimally invasive technique of cutting the UPJO via the urinary tract from the urethra. Acucise (Applied Medical, CA) is a ureteral cutting balloon which allows a retrograde placement of the catheter with the ability for simultaneous balloon dilation and incision of the ureteropelvic junction obstruction. The success rate of this procedure is 81-87.5%. The average operating time is 35-62.7 min. These procedures are performed under general, regional or intravenous sedation. The average hospital stay is 1.6-1.8 days with some patients treated successfully on an outpatient basis. The complication rate is 3.6-15.6%, which includes postoperative bleeding, hematuria, fever and ileus. This is a safe and effective treatment for the treatment of UPJO.
Advantages:
Unlike the antegrade endopyelotomy, a nephrostomy tract is not necessary. In addition, this procedure eliminates the complications of pneumothorax and hydrothorax.
This is a more rapid procedure, shorter hospital stay and less postoperative discomfort than antegrade endoscopic alternative.
Disadvantages:
Similar to antegrade endopyelotomy, fluoroscopic control is required. The major disadvantage is the need for placement of an indwelling ureteral stent. Blood loss may require the need for blood transfusion (1.5%) or embolization (3%).
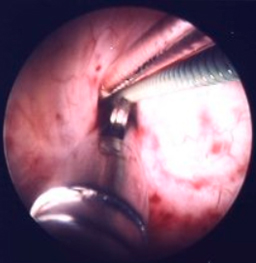
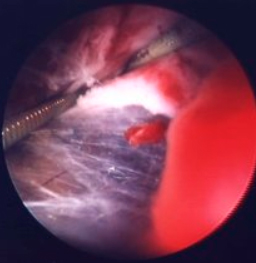
LAPAROSCOPIC PYELOPLASTY
The average operating time is 5 hours. The mean hospital stay is 3 days.
Advantages:
Can be done in patients with crossing lower pole vessels or large redundant pelvis.
Disadvantages:
Requires technical expertise.
Suggested readings
Faerber GA, Richardson TD, Farah N, Ohl DA. Retrograde treatment of ureteropelvic junction obstruction using the ureteral cutting balloon catheter. J Urol, 157:454-458.
Nadler RB, Rao GS, Pearle MS, Nakada SY, Clayman RV. Acucise endopyelotomy: assessment of long-term durability. J Urol, 156:1094-1098, 1996.
Motola JA, Badlani GH, Smith AD. Results of 212 consecutive endopyelotomies: an 8-year followup. J Urol, 149:453, 1993.